When facing long-term treatment for kidney failure, establishing reliable vascular access is paramount for successful and efficient therapy. The arteriovenous fistula definition describes a surgical procedure that creates a direct connection between an artery and a vein, typically in the arm. This connection is the single most effective method for creating a durable and reliable access point for hemodialysis.
At The Optimum Clinic, we emphasize this crucial first step. The AV fistula meaning embodies the best clinical practice: a long-lasting, low-complication vascular route that can withstand the rigors of repeated needle insertions necessary for renal replacement therapy.
An Arteriovenous fistula (AV) fistula is universally regarded as the best long-term vascular access for Hemodialysis for several key reasons:
Longevity: It ensures the access lasts for a longer period of time—often many years—with minimal need for intervention compared to grafts or catheters.
Reduced Complications: It has significantly fewer complications, such as infection, blood clots, and hospitalization, than other access types.
Optimal Flow: It guarantees sufficient, high-volume blood flow, which is essential for ensuring the hemodialysis machine efficiently cleanses the blood.
Creating a successful arteriovenous fistula for haemodialysis requires meticulous planning and execution. It is not an urgent procedure but one that requires strategic foresight, as a newly created fistula needs time to develop and strengthen—a process called "maturation."
Before the AV fistula operation, thorough assessment is mandatory. Once you are referred by your nephrologist for creation of AV fistula, you will be thoroughly assessed by our expert team:
Physical Examination: Evaluating the size and health of your veins and arteries.
Doppler Mapping: Using advanced ultrasound technology to precisely map the vessels in your arm. This detailed report helps Dr. Rajan Sharma determine the most suitable anatomical site for fistula creation based on vessel size and flow dynamics.
The AV fistula operation involves connecting an artery directly to an adjacent vein, quite often in the forearm or upper arm. This high-pressure arterial flow is diverted into the low-pressure vein, enhancing the vein's size and thickness over time. This surgery is typically performed using a local or regional anaesthetic.
A crucial aspect of planning is the maturation period. A fistula often takes some time after surgery to develop—usually 4 to 12 weeks. In due course, the vein grows larger and thicker, which in turn makes repeated needle insertions for the treatment easier and less traumatic. Patients and caregivers must be educated on protecting the fistula during this critical phase.
While the arteriovenous fistula for dialysis is the safest option, patients must remain vigilant about potential AV fistula complications. Early detection is key to maintaining access longevity. Common complications include:
Thrombosis (Clotting): The formation of a blood clot within the fistula, which blocks blood flow.
Stenosis (Narrowing): A localized narrowing of the vein, which restricts blood flow and affects dialysis efficiency.
Infection: Although rare, localized redness, pain, or swelling must be reported immediately.
Steal Syndrome: Occurs when too much blood is diverted to the fistula, leading to coldness, numbness, or pain in the fingers or hand.
For accurate diagnosis, referral, and comprehensive long-term care, medical records require precise coding. The AV fistula ICD 10 code (e.g., relating to Z49.0 for preparation for dialysis or I77.0 for the procedure itself) ensures consistent communication between the surgeon, nephrologist, and care facility, contributing to the highest standard of coordinated care.
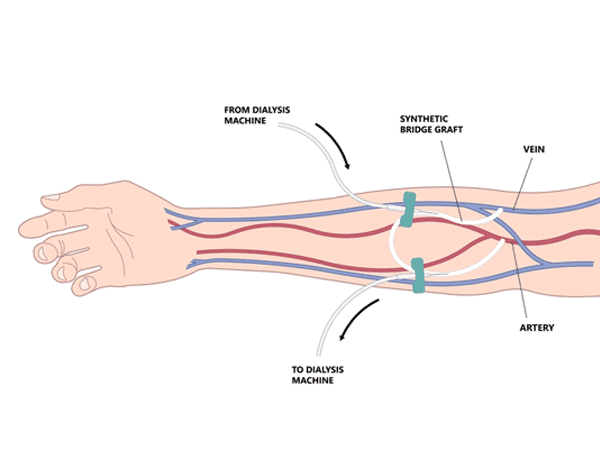
In situations where a patient's veins are too small, weak, or fragile, preventing them from achieving adequate maturation for a native AV fistula, an Arteriovenous Graft may be necessary.
If there are small veins that won’t develop into a native fistula, a vascular access is created using a graft—a synthetic tube—to connect the artery to a vein. This graft is implanted under the skin in your arm and acts as an artificial vein. The main benefit is that a graft could be used sooner after placement (often within 2-3 weeks) compared to an arteriovenous fistula. However, grafts are generally associated with a higher risk of infection and clotting.
Dr. Rajan Sharma and our specialized team are committed to providing you with the highest quality AV fistula operation and follow-up care. By utilizing Doppler ultrasound for detailed pre-operative planning and prioritizing the creation of a native arteriovenous fistula for dialysis, we maximize the lifespan and reliability of your vascular access, ensuring the smoothest and most efficient path to long-term renal replacement therapy.